
Uterine fibroids can be treated with radiological and other methods. These can include endometrial ablation, uterine artery embolization, magnetic resonance imaging–guided focused ultrasound, and myomectomy.
These treatments are minimally invasive and typically involve a short hospital stay or can be done as an outpatient procedure. Before undergoing any treatment for uterine fibroids, you should discuss your options with your health care provider.
Endometrial ablation (pronounced ah-BLAY-shun) destroys the lining of the uterus. It is used to treat small fibroids inside the uterus. Ablations can be performed in a variety of ways, including using electric currents, using microwave energy, and freezing.
Pregnancy is unlikely after this procedure, but it can happen. Women who get pregnant after endometrial ablation are at higher risk for miscarriage and other problems. If you are going to have this treatment, talk to your health care provider about the risks of getting pregnant after the procedure. You might want to use birth control to prevent pregnancy until after you go through menopause.1
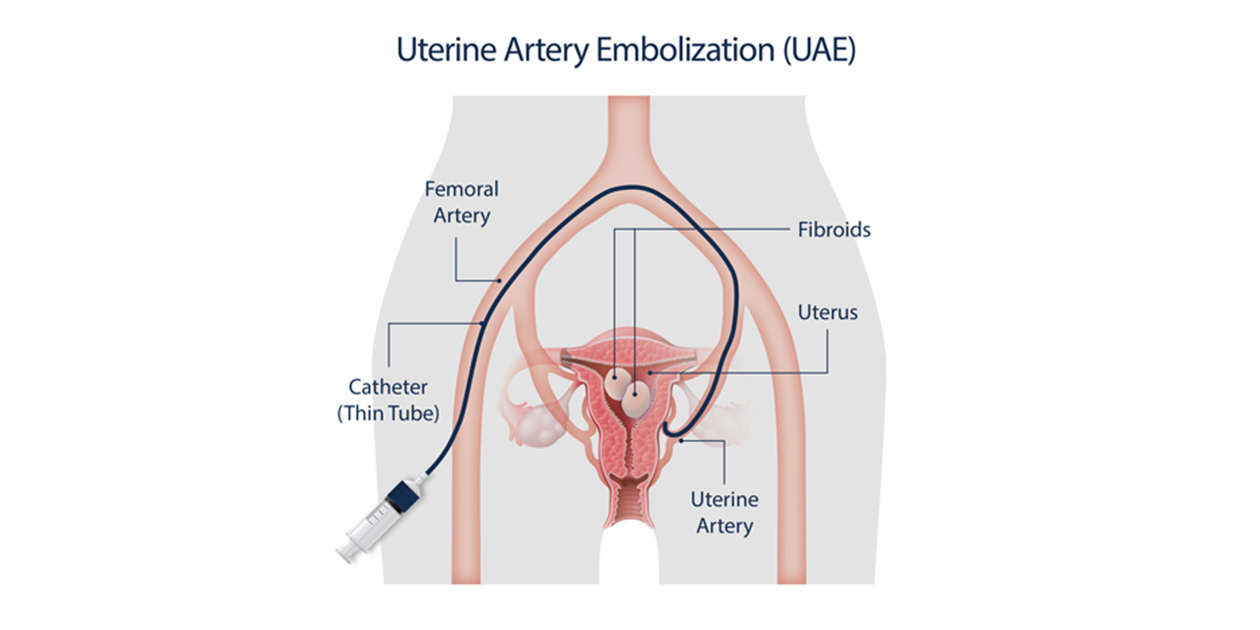
Uterine artery embolization (pronounced em-bohl-ih-ZAY-shun), or UAE, is also called uterine fibroid embolization (UFE).
In this procedure, the doctor makes a small cut in the groin area, inserts a tube (called a catheter) into the large blood vessel there, and slides the tube until it reaches the arteries that supply blood to the uterus. He or she then injects tiny plastic or gel particles through the tube into the arteries. The particles block blood flow to the fibroids, so they eventually shrink and may relieve symptoms.2
Some research has shown that UAE successfully treats fibroids but that about one-third of women who have UAE need treatment again within 5 years.3
Because this procedure stops blood flow to parts of the uterus, it can affect how the uterus functions. It can also affect how the ovaries function if the inserted particles drift into other areas of the pelvis, such as the ovarian artery. Its effect on pregnancy is not clear, but an increased risk of miscarriage has been reported. For this reason, most health care providers do not recommend UAE for women who want to have children.
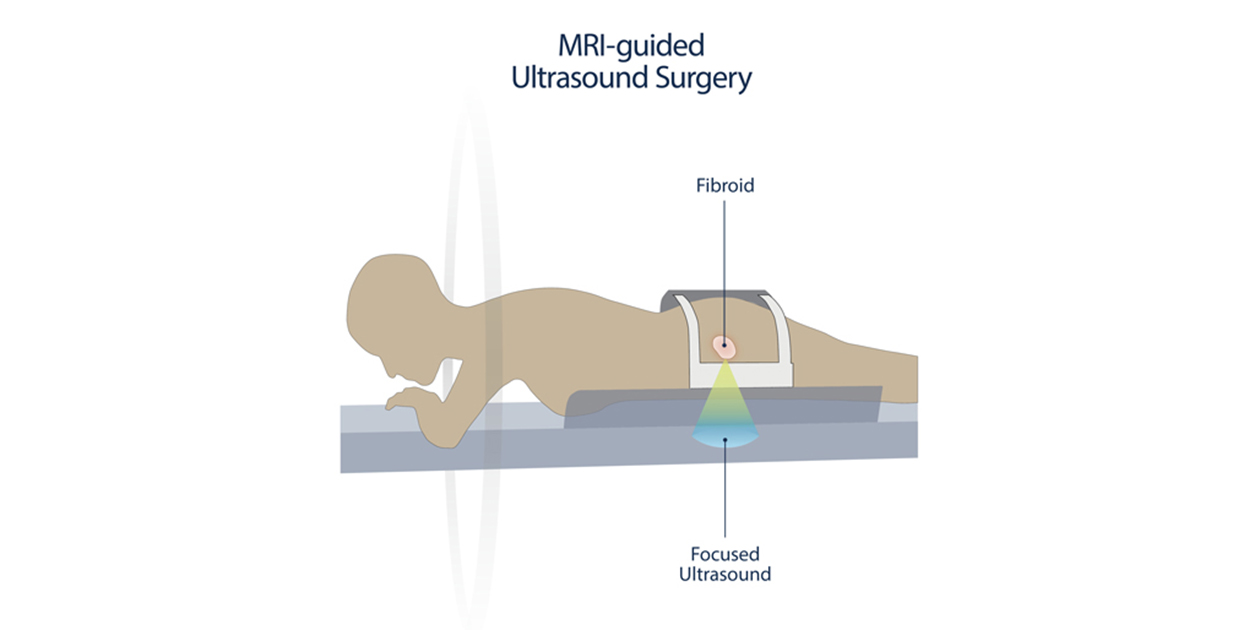
This treatment destroys fibroids by using high-intensity ultrasound. The health care provider uses an MRI scanner to see the fibroids and then directs focused ultrasound waves through the skin to destroy the fibroids. This option is usually recommended for women who have only a few large fibroids.4
Scientists are still studying the long-term effects of this procedure.4 Studies show that although symptoms improve up to a year after having MRI-guided focused ultrasound, within 2 years, about one in three women will need another surgery or another procedure to treat fibroids.4,5 Because MRI-guided focused ultrasound is a relatively new kind of treatment, your health care provider may not offer it, or your health insurance company may not pay for it. It may also affect how ovaries function.
Myomectomy is a surgical procedure that removes only the fibroids and leaves the healthy areas of the uterus intact. It can preserve the ability to get pregnant.
Myomectomy can be performed in one of three ways, depending on the location and size of the fibroids:
- Hysteroscopy (pronounced hiss-tur-AH-skoh-pee). For this procedure, the surgeon inserts a long, thin telescope with a light through the vagina and cervix (the opening of the uterus). The doctor then uses electricity or a mechanical device to cut or destroy the fibroids. The doctor will inject a fluid into the uterus to make it easier to see before trying to remove the fibroids.
- Laparotomy (pronounced lap-are-AH-toh-mee). The surgeon removes the fibroids through a cut in the abdomen.
- Laparoscopy (pronounced lap-are-AH-skoh-pee). The surgeon uses a long, thin telescope to see inside the pelvic area and then removes the fibroids using another tool. This procedure usually involves two small cuts in the abdomen.
Studies show that myomectomy can relieve fibroid-related symptoms in 80% to 90% of women.3 The original fibroids do not regrow after surgery, but new fibroids may develop.
What are the symptoms of uterine fibroids?
What are the risk factors for uterine fibroids?
 BACK TO TOP
BACK TO TOP