
BPCA exists to improve the safety and efficacy of drug use and dosage for children.
BPCA became law in 2002. It was reauthorized in 2007 under the U.S. Food and Drug Administration (FDA) Amendments Act, in 2012 under the FDA Safety and Innovation Act, and again in 2017 under the FDA Reauthorization Act. The latest renewal of the BPCA legislation occurred in 2022.
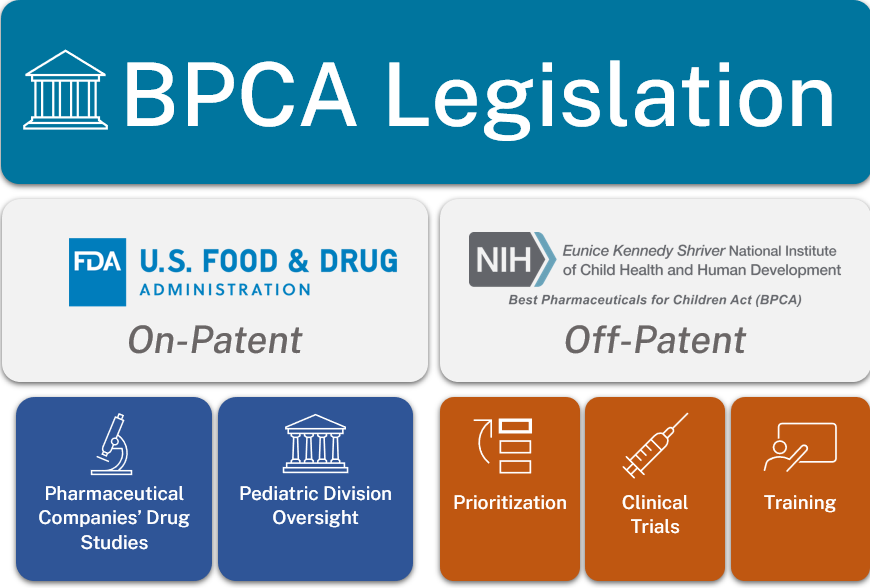
The overarching goals of BPCA are to:
- Encourage the pharmaceutical industry to perform pediatric studies to improve labeling for patented drug products used in children, by granting an additional 6 months of patent exclusivity
- Authorize NIH, through Section 409I, to prioritize needs in various therapeutic areas and sponsor clinical trials of off-patent drug products that need further study in children, as well as training and other research that addresses knowledge gaps in pediatric therapeutics
BPCA 2002
Established FDA Office of Pediatric Therapeutics
Established Pediatric Advisory Committee
NIH Mandate (409I) authorized NIH to:
- Prioritize testing of off-patent pediatric drugs
- Sponsor clinical trials and other research to provide data for prioritization (via contracts)
- Submit data to FDA for labeling change
BPCA 2007 (FDA Amendments Act)
Prioritization:
- Therapeutics focus
- Additional language regarding developmental pharmacology and infrastructure for trials (including training)
Trials:
- Flexibility in funding
- Proposed pediatric study requests
- Feasibility study
BPCA 2012 (FDA Safety and Innovation Act)
FDA's BPCA program made permanent
- Posting of medical reviews
- Development of pediatric study plans
NIH's BPCA program still requires renewal every 5 years
Neonates considered a priorityBPCA 2017 (FDA Reauthorization Act)
Data dissemination:
- NIH to post data on the NICHD Data and Specimen Hub (DASH) within 90 days after submission of the report to the FDA
Priorities:
- Allowing research priorities to include the identification of biomarkers for pediatric diseases and conditions
Far more drugs have been approved for clinical use in children since the passing of legislations such as BPCA and the Pediatric Research Equity Act. However, despite knowledge gains, there is still a notable degree of off-label drug use for children who need treatment for various medical conditions. Use of drugs outside of the prescribed label indications is considered “off-label” use, which can lead to inadequate understanding of appropriate dose, safety, or efficacy. BPCA's role is to identify and address these knowledge gaps.
NIH implements the BPCA mandate by conducting the following activities:
- Identifying drugs (primarily off-patent drugs) that need to be studied in children due to lack of dosing, safety, or efficacy data
- Sponsoring clinical trials for those drugs, which includes:
- Identifying appropriate investigators and clinical sites to conduct these studies
- Carefully monitoring drug labeling studies in children
- Submitting study data to the FDA for consideration of label modification
- Making the study data available to researchers and the public
Congress authorizes approximately $25 million from the NIH budget each fiscal year for the operation of the BPCA program. NICHD contributes approximately 25% of BPCA funding from its annual budget. The remaining funds are drawn from more than 20 other NIH institutes with significant pediatric research portfolios.
 BACK TO TOP
BACK TO TOP